- Medical Matters
Contraception Use, Effectiveness and Adverse Effects
by Robert Chasuk, MD
CANFP NEWS Winter 2026
The topic of contraception methods in use today is quite broad, so this short article will be a high-altitude overview with a noticeably colorless style, which may best suit it.
There are four major categories of modern contraception: hormonal, long-acting reversible contraceptives (LARCs), barrier methods and permanent sterilization. This article will not discuss natural or fertility appreciation based methods.
Hormonal methods
include combined hormonal contraceptives or CHCs (pills, transdermal patches, vaginal rings containing estrogen plus progestin) and progestin-only methods (pills, injections, implants, and hormonal intrauterine devices (IUDs).
Long-acting reversible contraceptives (LARCs)
are becoming more popular and include intrauterine devices (hormonal and copper) and progestin-containing implants.
Barrier methods
include male and female condoms, diaphragms, spermicides.
Permanent methods
consist of female sterilization (tubal ligation) and male sterilization (vasectomy).
It is an obvious statement to say that use of contraception is widespread. In the United States, around 50% of women of reproductive age currently use some form of contraception. The most common methods include:
- oral contraceptive pills ~11%
- female sterilization ~11%
- long-acting reversible contraceptives (LARCs) ~10%
- male condoms ~7.1%
Adolescents ages 15-19 prefer condoms and oral contraceptive pills, while women 20-49 years favor LARCs, and female sterilization becomes more frequent in older women.
CHCs that contain both an estrogen and a progestin were initially developed in the 1960’s. Over time, newer estrogen and progesterone forms have been introduced, with trends toward lower doses, to ameliorate the serious adverse effects of these chemicals.
Contraceptive mechanisms can be described as acting pre-fertilization or or post-fertilization. Fertilization is the moment of the creation of a new human being (there is no such thing as a fertilized egg!) and most commonly occurs in the fallopian tube. The new embryo takes five to nine days to migrate to the uterus, where it can implant.
Post-fertilization mechanisms, then, essentially destroy a human being.
CHCs prevent uterine pregnancy by at least three and possibly four mechanisms. Two of these happen before fertilization: suppressing ovulation or altering cervical mucus or fallopian tube function to prevent sperm survival and transport. The other two mechanisms work after fertilization altering the lining of the uterus to be less favorable for implantation of the embryo and perhaps also by changing the properties of the fallopian tube that facilitate the migration of the embryo to the uterus for implantation.
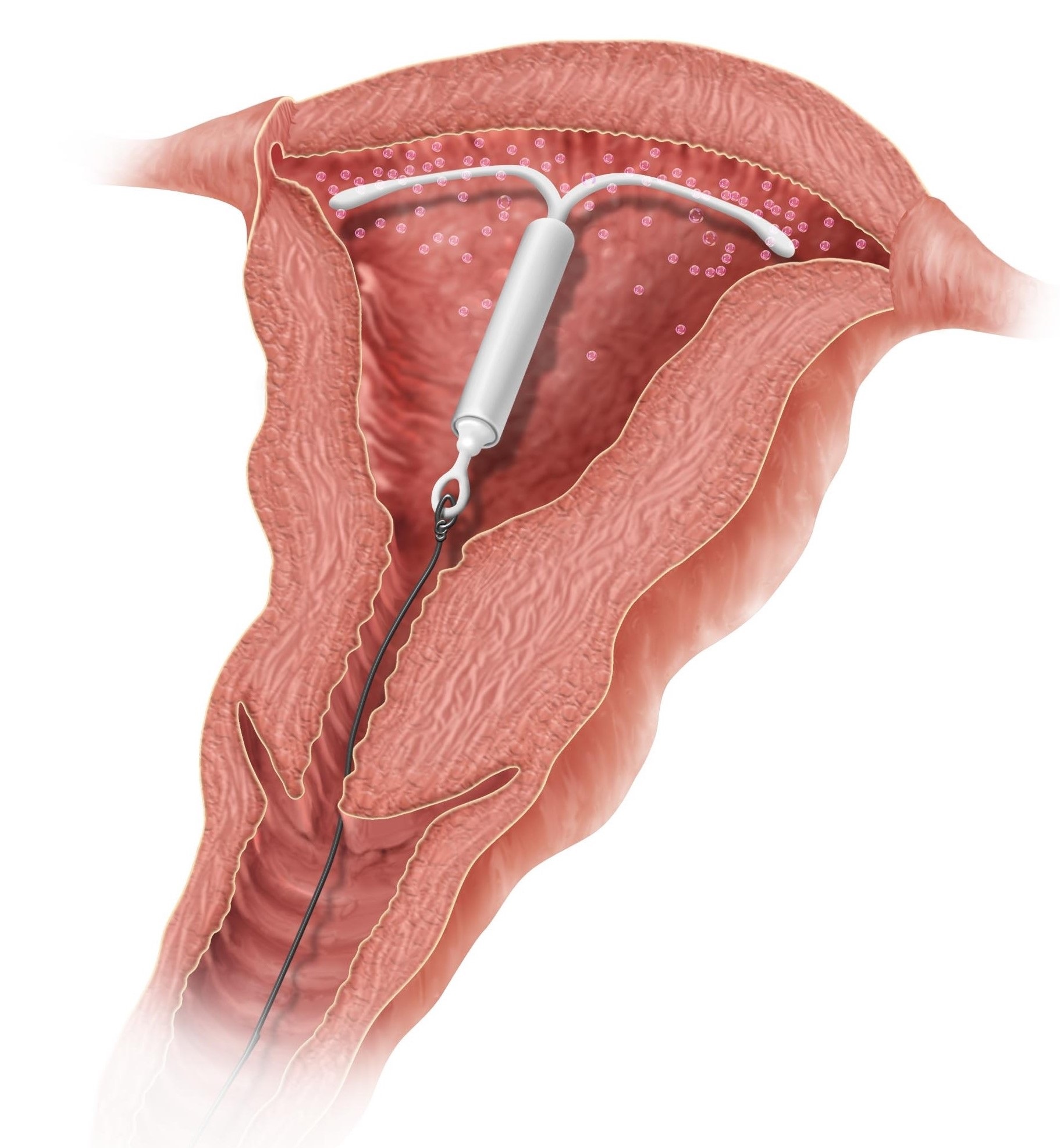
IUDs also have multiple possible mechanisms. Pre-fertilization mechanisms include inhibiting sperm or egg transport in the fallopian tubes. Post-fertilization mechanisms include inducing an unfavorable inflammatory environment in the reproductive organs that could prevent implantation or damage the embryo before implantation. Neither the progestin nor copper IUD suppress ovulation. IUDs decrease the overall rate of pregnancy, but if there is a breakthrough pregnancy, 25-50% will be ectopic (in the fallopian tube), demonstrating the IUD’s effectiveness of preventing intrauterine implantation (postfertilization) more effectively than extrauterine implantation.
Contraceptive methods vary in their effectiveness. A useful statistic is the percentage of women who will achieve an unintended pregnancy in the first typical year of use. The CDC reports the following rates:
- male condom 18%
- hormonal pills, transdermal patch, and vaginal ring device all 9%
- Copper IUD 0.8%
- Progestin IUD 0.2%
- subcutaneous progestin implant 0.05%
- female sterilization 0.5%
- male sterilization 0.15%
Serious adverse effects of contraception include venous thromboembolism, breast and cervical cancer.
Women taking CHCs have a three to five times greater risk of venous or pulmonary thromboembolism, which equals around one additional death per 6,000 women taking them for a year. If a woman is a smoker, the risk increases to one additional death per 250 women-years. The highest risk is for those CHCs containing desogestrel, gestodene, drospirenone or cyproterone acetate. The risk increases 35 times in a woman who has the clotting disorder called Factor V Leiden, which is present in 5% of Caucasians.
CHCs are promoted for decreasing the incidence of ovarian and uterine cancer. But CHCs increase the risk of breast cancer, and the overall rate of breast cancer is six times that of ovarian and uterine cancer. Breast cancer risk increases 40-50% when CHCs are used before the first full-term pregnancy. The risk of triple negative breast cancer, which is particularly hard to treat, increases 2.5-fold with greater than one year of use of CHCs and more than 4-fold if started before the age of 40.
CHCs are a risk factor for cervical cancer. After ten years of use by women 20-30 years old, there is one additional case of invasive cervical cancer for every 1,400 women.
There is insufficient long-term evidence to conclude that the most recent CHCs with newer estrogen formulations, such as estetrol, reduce the risk of these adverse effects.
There have been reports about the effect of hormonal contraceptives on women’s mate preferences and relationship satisfaction, but the evidence is not conclusive.
Considering the possibly life-threatening adverse effects of CHCs, wouldn’t it be great if there were a real birth regulation method that was effective in avoiding or achieving pregnancy without side effects? Of course, there is with natural family planning

About The Author
Robert Chasuk, MD
