- Medical Matters
Oral Contraceptives & Adolescents——Impact on Mood and Risk of Mental Disorders
by Lauren Rubal, MD, FACOG
Being a teenage girl is tough. As an adolescent, I remember a multitude of social, academic, and extracurricular pressures, and this was decades before TikTok, Instagram, and YouTube channels.
The adolescent years are also a time of formation in every possible facet. Of course, the physical changes are profound, and they are only exceeded by the growth in responsibility (I don’t know how my mother was able to take all my erratic attempts at learning how to drive!). Physiologically, the brain experiences a high degree of plasticity during this time (similar to that found as a baby), meaning that many neuronal connections are developing, growing and shifting. And the spiritual formation is the most important of all, as teens are confronted with many temptations and challenges to their faith.
So how can we best set up our teenagers to succeed? Studies show this is a critical question, as the rates of teenage depression, anxiety, and suicide have all risen dramatically.
Of course, continued catechesis to promote a deepening of character and values is the most important. But society clearly impacts our children. And do you know who else does? Doctors — specifically gynecologists and pediatricians. Every woman will be counseled by one of these types of physicians multiple times in their lives. These physicians provide much good. But unfortunately our field as a whole has normalized and equated oral contraceptive pills (OCPs) to a sort of prescribed candy. 44% of sexually active 15 to 19 year old girls are using OCPs. When one considers that about half of teens are sexually active, and that there are 12 million teen girls in the United States, the sheer number of adolescents using OCPs is staggering.
And hormones are powerful. Any woman who has experienced the shifts of pregnancy, menopause, or even a typical menstrual cycle can attest to this. Hormones can exert many different effects because they have receptors in multiple organs. One of these organs is the brain. In fact, hormones can alter the action of neurotransmitters, which ultimately can affect memory, learning, mood, sleep/wake cycles, reward pathways, decision making, and motivation.
A recent study used functional MRI imaging to examine brain activity and mood response to a psychological stressor during times of both high and low estrogen within the cycles of ovulating women. The group found that high estrogen decreased subjective distress as well as activation of corresponding brain areas on imaging compared with a low estrogen state.
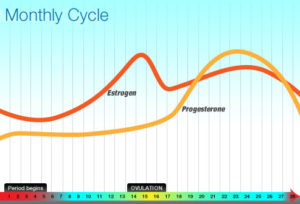
There is also evidence that the sequence and combination of hormones given may lead to quite varied effects. This is important because in the normal ovulatory cycle, a rise in unopposed estrogen precedes the subsequent increase in post-ovulatory progesterone, followed by a two-week plateau of both hormones together. There is a cyclicity within the menstrual cycle that is fundamentally at odds with the flatline produced by both combination OCPs (composed of synthetic estrogen and progesterone), and progestin only OCPs. OCPs are progestin-dominant, meaning that though a synthetic estrogen and progesterone are given with combination pills, it is the progestin effects that are most pronounced. Thus, there is no cycling at all; both estrogen and progesterone are administered in tandem for the entire month with progestins exerting an unceasing dominance. This matters because estrogen is the hormone associated with positive cognitive effects such as well-being, improved memory and attention, and decision-making ability. On the other hand, non-cyclic progesterone and its metabolites increase depression and irritability.
The end result in the brain is a relatively low estrogen milieu with no break from progesterone—the perfect storm for development or exacerbation of mood disorders.
In Denmark, a population cohort study examining over one million women from age 15 to 34 years old showed that amongst users of any type of hormonal contraception, there was an increased risk of subsequent development of first diagnosis of depression or first use of anti-depressants. These risks were increased compared to non-users with each contraceptive method and the highest risks (approximately double) were noted in girls 15 to 19 years old.
A subsequent study by the same group followed about half a million women with an average age of 21 and for an average of eight years with no prior diagnosis of mood disorder. They found an increased risk (up to three-fold, even after adjusting for other risk factors) of suicide and attempted suicide with ever use of hormonal contraception.
The takeaway? Teenagers have many psychological challenges. Many are offered OCPs during doctor appointments for varied causes, both gynecologic and contraceptive. OCPs then induce essentially the opposite hormone milieu in the brain compared to a normal ovulatory cycle. This results in an overall low estrogen state as well as predominant and unchanging progestogen levels. Due to this, there may be an increased risk of new onset depression and even suicide. This may persist even after stopping the OCPs, possibly due to the increased brain plasticity that occurs during this age.
Let’s help our teens and avoid these powerful medications. Discussing abstinence with teens has been shown to improve compliance with avoiding intercourse. In this way, we can best protect and safeguard our teens during the last phase before independent adulthood.
References
Helping teenagers postpone sexual involvement.Howard M, McCabe JBFam Plann Perspect. 1990 Jan-Feb; 22(1):21-6.
Trends in contraceptive use in the United States: 1982-1995.Piccinino LJ, Mosher WDFam Plann Perspect. 1998 Jan-Feb; 30(1):4-10, 46.
Davtyan C. Evidence-based case review. Contraception for adolescents. West J Med. 2000;172(3):166-171. doi:10.1136/ewjm.172.3.166
Albert K, Pruessner J, Newhouse P. Estradiol levels modulate brain activity and negative responses to psychosocial stress across the menstrual cycle. Psychoneuroendocrinology. 2015 Sep;59:14-24. doi: 10.1016/j.psyneuen.2015.04.022. Epub 2015 May 7. PMID: 26123902; PMCID: PMC4492530.
Del Río JP, Alliende MI, Molina N, Serrano FG, Molina S, Vigil P. Steroid Hormones and Their Action in Women’s Brains: The Importance of Hormonal Balance. Front Public Health. 2018 May 23;6:141. doi: 10.3389/fpubh.2018.00141. PMID: 29876339; PMCID: PMC5974145.
Andreano JM, Touroutoglou A, Dickerson B, Barrett LF. Hormonal Cycles, Brain Network Connectivity, and Windows of Vulnerability to Affective Disorder. Trends Neurosci. 2018 Oct;41(10):660-676. doi: 10.1016/j.tins.2018.08.007. Epub 2018 Sep 25. PMID: 30274602; PMCID: PMC6481680.
Rapkin AJ, Morgan M, Sogliano C, Biggio G, Concas A. Decreased neuroactive steroids induced by combined oral contraceptive pills are not associated with mood changes. Fertil Steril. 2006 May;85(5):1371-8. doi: 10.1016/j.fertnstert.2005.10.031. Epub 2006 Apr 3. PMID: 16580672.
Skovlund CW, Mørch LS, Kessing LV, Lidegaard Ø. Association of Hormonal Contraception With Depression. JAMA Psychiatry. 2016 Nov 1;73(11):1154-1162. doi: 10.1001/jamapsychiatry.2016.2387. Erratum in: JAMA Psychiatry. 2017 Jul 1;74(7):764. PMID: 27680324.
Skovlund CW, Mørch LS, Kessing LV, Lange T, Lidegaard Ø. Association of Hormonal Contraception With Suicide Attempts and Suicides. Am J Psychiatry. 2018 Apr 1;175(4):336-342. doi: 10.1176/appi.ajp.2017.17060616. Epub 2017 Nov 17. PMID: 29145752.
About The Author

Lauren Rubal, MD, FACOG
