- Medical Matters
Tube Trouble?
by Amie Holmes, MD, OBGYN, NaPro Surgeon
Fallopian tubes are delicate structures that connect the uterus to the pelvic space, or peritoneal cavity. They are passageways for sperm and eggs and provide a location for fertilization. They direct the fertilized embryo to the uterus where implantation usually occurs.
The fallopian tube is divided into four parts. In order, from the uterine opening (ostium) to the farthest end, these are called the isthmus, ampulla, infundibulum and fimbriae. The proximal tube (the portion closest to the uterus) has a very thin central lumen; the farthest part (the fimbriae) has fingerlike projections near the ovary that collect the egg after it is released from the ovary (ovulation).
“Tubal factor” refers to disease of the fallopian tubes that results in infertility. It is estimated that 25-35% of female infertility is caused by tubal factor. There are several causes of tubal factor infertility.
Most tubal disease is a result of inflammation. The most common cause of pelvic inflammation is infection. Sexually transmitted infections, such as chlamydia and gonorrhea, can cause pelvic inflammatory disease (PID). The inflammation causes scar tissue on the inside and the outside of the tubes. Swelling of the tube can result when the end of the tube is blocked and the tube fills with inflammatory fluid. It is estimated that one episode of PID leads to an 8% risk of infertility. After three episodes of PID, there is a 40% risk of infertility.
Abdominal infections, such as appendicitis, or abdominal or pelvic surgery can result in adhesions. Adhesions are internal scar tissue, which cause tissues and organs to stick together abnormally. When adhesions are near or around the tube they can cause a partial or complete tubal blockage. Pelvic endometriosis is an inflammatory condition where plaques of endometrial cells (normally inside the uterus) invade the pelvis. Endometriosis can adhere to the tube and cause adhesions leading to tubal blockage.
Another cause of tubal blockage is from uterine masses, such as fibroids, which can occasionally block the uterine opening to the tube (ostium). A more uncommon cause of tubal disease is Salpingitis Isthmica Nodosum (SIN), where nodules form throughout the tube and obstruct the lumen. The cause of SIN is unknown; however, theories suggest both congenital and inflammatory etiologies.
Unfortunately, many reproductive specialists will recommend in-vitro fertilization (IVF) in patients with tubal disease. Many patients are opposed to IVF for moral and ethical reasons as this eliminates the gift of natural conception between spouses from the process. It also results in extra embryos that must be either frozen or discarded. IVF does not correct the underlying cause of infertility. Any symptoms associated with the underlying disease are ignored. Additionally, this technique is very expensive.
The good news is that there are many ways to repair and open tubes! The success rates are often very good using highly specialized procedural and surgical techniques. The chances for pregnancy are often better than the rates achieved by IVF. Furthermore, correcting the underlying disease offers the potential for additional pregnancies over the reproductive lifespan and can resolve symptoms associated with the disease. These techniques are frequently more affordable as well.
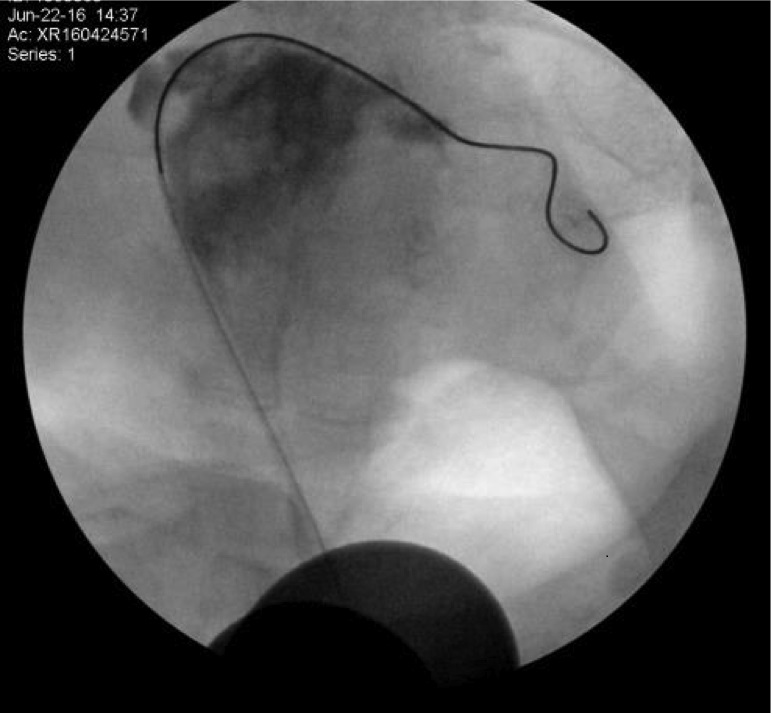
NaPro Technology focuses on repairing the tube utilizing several different techniques. “Selective” hysterosalpingogram is a specific way of evaluating the tube by injecting dye through a small cannula that is passed into the uterus through the cervical opening and then into the opening of the tube. Dye is injected while the tubal pressure is measured, and fluoroscopy (x-rays) outlines the tubes. If the dye doesn’t spill through the tube or if the pressure is elevated, a flexible guidewire is threaded through the tube to open up the blockage. Success rates range from 58-93% (depending on the degree and cause of blockage), and pregnancy rates are around 60%. This procedure gives a more accurate assessment and provides a therapeutic treatment as opposed to a traditional hysterosalpingogram, where dye is injected through the cervix into the uterus and x-ray pictures look for tubal spillage.
NaPro uses minimally invasive surgery to divide tubal adhesions through laparoscopy and robotic surgery. Robotic surgery allows for microsurgical techniques to be applied to the tube. Fimbrioplasty is a procedure that opens up the end of a blocked tube. Tubal reanastamosis involves removing an occluded portion of the tube and reconnecting the open portions. This technique can also be used to reverse tubal ligations. A high percentage of women who have had a tubal ligation later regret their decision. Some develop a painful condition known as “post-tubal ligation syndrome.” Robotic tubal ligation reversal has shown excellent success rates in early studies.
Often women with tubal disease experience pain and irregular bleeding. Correcting the underlying cause often results in improved health and well-being. Consulting with a NaPro specialist will allow you to discuss options for tubal repair and reconstruction
RESOURCES
Bolaji, Oktaba, Mohee, Sze, “An odyssey through salpingitis isthmica nodosa,” European Journal of Obstetrics & Gynecology and Reproductive Biology, 184, 2015.
Cobellis et al, “Selective salpingography: preliminary experience of an office operative option for proximal tubal recanalization,” European Journal of Obstetrics & Gynecology and Reproductive Biology 163, 2012.
Hafner, “Pathogenesis of fallopian tube damage caused by Chlamydia trachomatis infection,” Contraception, 92, 2015.
Kuzmin and Linde, “Diagnostic and remedial capability of transcervical falloposcopy in conjunction with laparoscopy,” Gynec Endocrinol, 30, 2015.
Lazer et al., “The place of selective hysterosalpingography and tubal canalization among sub-fertile patients diagnosed with proximal tubal occlusion,” Arch Gynecol Obstet, 293, 2016.
Robotic-assisted laparoscopic microsurgical tubal anastomosis: a human pilot study.” Fertility and Sterility, Vol 73, Issue 5, May 2000

About The Author

Amie Holmes, MD, OBGYN, NaPro Surgeon
